Nein Nine
Or so I thought, as Tina and I drove to Champalimaud for the surgeon consultation.Last week I did the imaging — a CT and an MRI — and we'd been waiting on the read. My oncologist called at the end of the day yesterday. Five minutes. She was canceling chemo #9 because the tumors had shrunk, canceling our meeting, and leaving me with just the surgeon consult.
I asked if she could email me the radiologist's report. Not complete yet. So I'd walk into the surgeon meeting without knowing how much things had moved.
Pre-game
This morning, I pulled up my own Surgeon Rankings page to re-read the questions I'd written for these consultations. I'm glad I built that page for reference. I stopped shopping for surgeons in the US after hitting too many walls — insurance, geography, second-opinion lag — and rooted instead for the surgeon in front of me to pass my interview.He did.
Meeting Dr. Cunha
Tina and I walked in. Dr. José Filipe Cunha introduced himself, and I was taken aback by his age. I'm not sure why I was expecting someone younger, but a seasoned surgeon is what you want.He came prepared. Knew my case. Walked us through the process, the warnings and the realistic timeline.
I asked how many of these he's done.
One to two per week.
How many total?
I stopped counting.
I pushed — over 200?
Yes. Well over 200.
He's been performing this procedure in Portugal since 2003 — one of the first. He'd be operating with a team of five surgeons.
That's the answer I came for.
What CRS+HIPEC actually is
For anyone new to this site: I'm being evaluated for CRS+HIPEC — Cytoreductive Surgery plus Hyperthermic Intraperitoneal Chemotherapy. It's the standard-of-care treatment for peritoneal carcinomatosis (cancer cells that have seeded the lining of the abdomen).The surgery is two procedures stacked back-to-back:
CRS — the surgeon opens the abdomen and physically removes every visible tumor, along with any tissue or organs the cancer has touched. Peritonectomy means stripping out the peritoneum, the thin tissue lining the abdominal cavity, in the regions where disease is present.
HIPEC — once everything visible is out, heated chemotherapy is pumped into the abdomen and circulated for 90 minutes. The heat (around 41–43°C) amplifies the chemo's ability to kill microscopic disease the surgeon couldn't see. Then it's drained, the patient is closed, and recovery begins.
This is not a maintenance therapy. It's a one-shot at curative intent.
The timeline he laid out
Laparoscopy first, same surgery. Some programs do a separate diagnostic laparoscopy weeks earlier to assess the disease burden. Dr. Cunha does it at the start of the same operation. If what he sees inside doesn't match the imaging, he can adjust or abort without me having already gone under twice.Surgery block:
- 1 hour prep
- 5 hours laparoscopy + CRS
- 1 hour HIPEC setup
- 90 minutes of heated chemo circulating in my abdomen
- ICU: 1–3 days
- Hospital total: ~10 days
- Back to almost normal: 1–2 months
The scan results, finally
I asked how much the lesions had shrunk. He pulled up the scans.Two of the four are almost invisible.
He didn't give me exact numbers, but "almost invisible" is the word I needed. The FOLFIRI is doing its job.
The timing conversation came next
The standard protocol is four weeks between the last chemo and surgery. But I'm receiving bevacizumab — Avastin — as part of my FOLFIRI cocktail. Bevacizumab is a monoclonal antibody that blocks the tumor's ability to grow new blood vessels. Useful for starving cancer. Less useful when a surgeon is trying to cut into you and have things heal afterward. It interferes with wound healing and raises the risk of bleeding complications, so they want it fully cleared before opening the abdomen. That pushes the gap to eight weeks.My last chemo, number 8, was two weeks ago. Six weeks out puts us at the end of June. I was prepared for roughly that window.
But I had an important date: July 10th. NOS Alive. Soren, Tina and I have tickets to see the Foo Fighters — his first time seeing them, and he's been counting down for months.
I asked Dr. Cunha if there'd be any harm in pushing the surgery out two more weeks so I could do this thing with my family.
He thought about it. I don't think so.
I pushed a little. Any concern about waiting that long? Any window where the cancer could start growing back?
Another pause. Then: if I wanted to push to ten weeks, he'd suggest one more round of chemo — without the bevacizumab — to keep the disease suppressed through the longer wait.
I said yes immediately. Another round of chemo is a fair price to see the Foo Fighters with my son.
He went to find my oncologist. She was in another consultation, so she'll call me tomorrow. I'm assuming I'm back on for chemo #9, which technically kills the title of this post.
I'm keeping the title anyway. I already liked the wordplay.
The gallbladder goes too
While he's in there, he'll take out my gallbladder. I have gallstones, and once the abdomen is open, it would be malpractice not to. The gallbladder is a small sac under the liver that stores bile — the fluid that helps you digest fats. You can live without it. The liver delivers bile directly to the small intestine rather than storing it. Most people adjust without issue; some have to back off greasy meals for a while.My organ inventory, post-surgery:
- Appendix — gone (2024, the perforation that started all of this)
- Thyroid — half gone (2019)
- Colon — half gone (2024)
- Gallbladder — gone (soon)
The formal surgical proposal
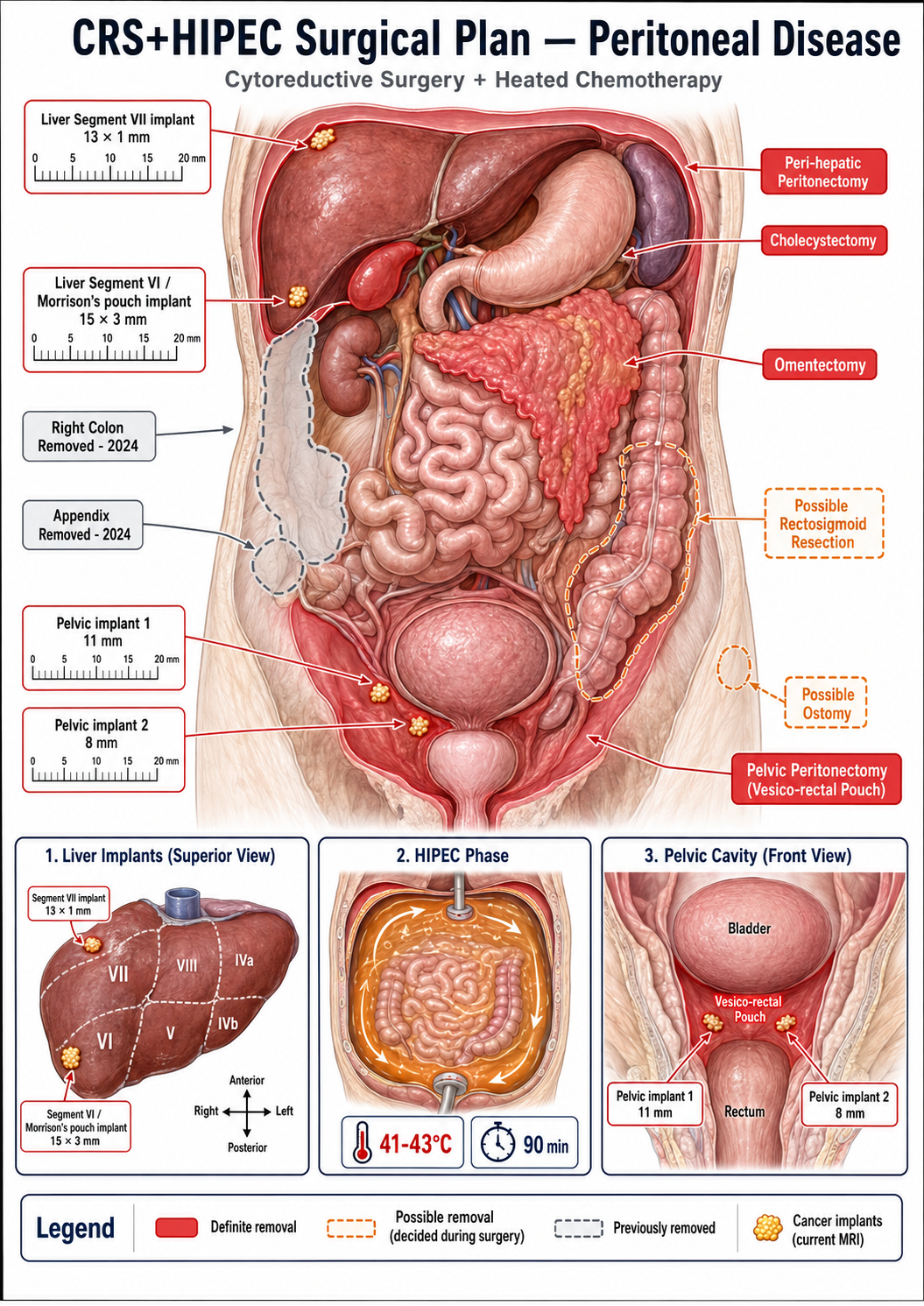
The plan, in their words: cytoreductive surgery and HIPEC for peritoneal metastases of adenocarcinoma of the cecum, plus removal of the gallbladder for gallstones.Based on the imaging, the plan includes:
- Peritonectomy in the peri-hepatic region (around the liver) and pelvis
- Omentectomy — removal of the omentum, the fatty apron of tissue that hangs in front of the intestines; it's a common landing spot for peritoneal disease
- Cholecystectomy — gallbladder removal
- Excision of peritoneal lesions in the vesico-rectal pouch (the low pelvic space between the bladder and rectum)
- Possible rectosigmoid resection — removal of a section of the lower colon — and possible ostomy (rerouting the bowel to an opening on the abdominal wall) if the disease in that area is more extensive than the scans suggest
After chemo #9, the focus shifts. Nine weeks of summer to build my body back up, eat well, see the Foo Fighters with Soren, and stack the deck for what's coming. The rest of the year goes to recovery.